Bariatric and Metabolic Surgery
Currently, bariatric and metabolic surgery is the treatment of choice for severe obesity as it is the only proven method of intervention for significant weight reduction and long-term maintenance. People that elect this surgery have a high success rate of losing weight also achieving a high percentage of resolution or improvement of associated comorbidities.
Goals of bariatric and metabolic surgery:
Who is a candidate for metabolic and bariatric surgery?
- Non-responder of previous medical treatments (diet, exercise, changes in habits, weight loss medications).
- No indication of active alcoholism, active drug addiction or a major psychiatric disorder.
- BMI greater than 35 kg/m2
- BMI greater than 30 kg/m2 associated with diabetes, high blood pressure, sleep apnea, serious joint diseases, dyslipidemia, or fatty liver.
How do we perform bariatric and metabolic surgery?
All the bariatric and metabolic surgery we performed by video laparoscopy or minimally invasive surgery (through small cuts in the skin less than 1.2 cm), this means:
- Greater safety compared to traditional surgery
- Less painful
- It has fewer complications
- The patient is quickly mobile, walking two hours after surgery
- 1 day of hospitalization
- Quick return to work (6th day)

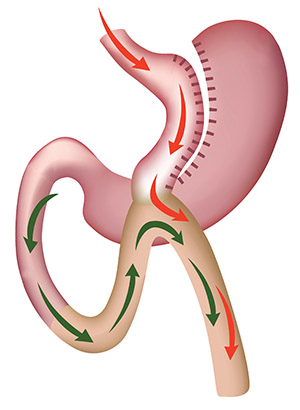
Roux-en-Y Gastric Bypass (Since 1966)
The size of the stomach is reduced to 40cc, the small intestine is skipped 2 meters (usual length 7 meters) and 2 anatomosis or connection are made (stomach-intestine and intestine-intestine) this produces a decrease in ghrelin (hunger hormone), an increase in incretins (GLP1, GYY hormones that help improve or resolve diabetes and hypertension) and generates a slight malabsorption (does not cause diarrhea).
Benefits
- 80% success.
- It is the one that provides the patient with the most tools (restriction, malabsorption and hormonal improvement).
- High percentage of disease resolution (see image).
Disadvantages
- Intestinal obstruction (0.6%), its requires surgery to resolve.
One Anastomosis Gastric Bypass OAGB (Since 2001)
The size of the stomach is reduced to 150cc, the small intestine is skipped 3 to 4 meters and only one anastomosis is made between the stomach and the intestine.
Benefits
- 85-90% success.
- Better effect in patients with BMI greater than 50.
- High percentage of disease resolution.
Disadvantages
- Two to three stools daily.
- You can develop gastro-esophageal reflux in 3%.
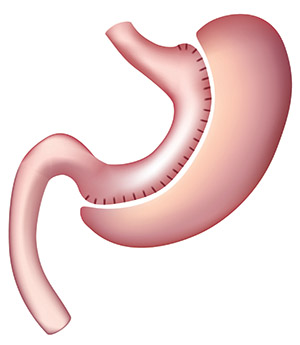
Gastric Sleeve or Sleeve gastrectomy (2003)
90% of the stomach is removed, reducing its capacity to 200 cc and by removing that part of the stomach that has most of the cells that produce ghrelin (hunger hormone), appetite is significantly reduced.
Benefits
- 68% success
- Resolution of obesity relative diseases, but 15 to 20% less than in gastric bypass.
- Recommended in patients with pre-malignant gastric lesions, with intestinal diseases or with intestinal adhesions due to major abdominal surgeries previously performed.
Disadvantages
- Development of gastroesophageal reflux after surgery between 5 to 20%.
- Weight regain in patients with BMI greater than 43.
The benefits of bariatric and metabolic surgery will depend on the surgical technique that is performed. In general, the obtained percentage of excess weight loss is between 68 to 85% (a significant difference, when compared to non-surgical treatment, which is only 5 to 15% in the best of cases).
In addition, there provide a resolution or improvement of diabetes in 85%; of arterial hypertension in 70%; dyslipidemia 85%; fatty liver by 90%; and sleep apnea by 95%.
What are the possible complications?
As in all highly complex surgeries, there are major complications (1.4%, which could require hospitalization) and minor complications (less than 4%).
- Early (7 days): Leakage < 1%, hemorrhage 0.8%, deep vein thrombosis 0.3%. They require hospitalization.
- Medium term (45 days):stenosis (shrinks) of the connection between stomach and intestine, it is simply resolved with endoscopy.
- Late (after one year):Vitamin deficiency (avoided by taking daily vitamin complex) and gallstone formation.
Mortality: It is 0.11%, less than that of a cholecystectomy (removal of the gallbladder).
In an obese patient, the risk of death due to not undergoing surgery is greater than the risk of possible complications after the surgical procedure.
Hospital Universitario Austral | Bariatric and Metabolic Surgery